Improved intraocular foreign body localization using orbital computed tomography data
DOI:
https://doi.org/10.31288/oftalmolzh202362832Keywords:
penetrating eye injury, intraocular foreign body, diagnostic imaging, computed tomographyAbstract
Background: Detection and localization of an intraocular foreign body (IOFB) are essential for assessing the severity of injury and selecting an appropriate method for IOFB removal.
Purpose: To improve the method of IOFB localization through the use of the Komberg-Baltin prosthesis while performing orbital computed tomography (CT) scans.
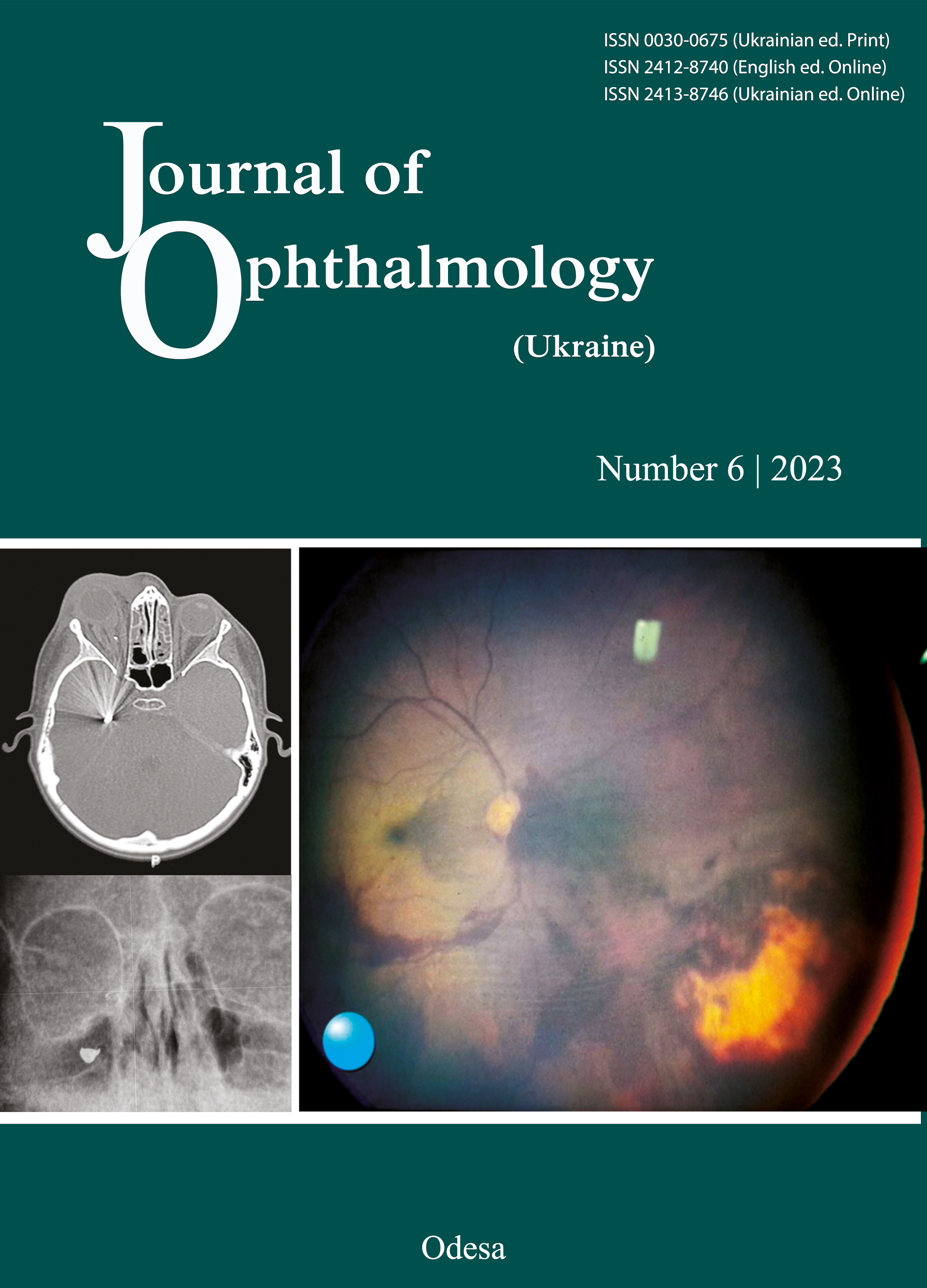
Material and Methods: We reviewed the medical records of 6 patients with a penetrating corneal and/or scleral injury and an IOFB in the posterior segment. Patients had ultrasonography of the ocular anterior and posterior segments and Komberg-Baltin prosthesis-assisted CT of the orbit as per our method reported previously to verify the location of the IOFB. Orbital radiography was performed at the point of care. The results of radiography, ultrasonography and CT for each case were reviewed and compared. The final verification of IOFB location was performed preoperatively during a standard three-port 25-G pars plana vitrectomy with IOFB removal.
Results: In 3 cases, intraoperative visualization during vitrectomy confirmed the results of preoperative IOFB imaging (radiography, ultrasonography and orbital CT). In these cases, an IOFB was a metallic fragment measuring 0.9 to 2.5 mm. In one case, a metallic IOFB was found by ultrasonography, but not by radiography. CT, when performed by our method, found an IOFB measuring 0.2 x 0.3 mm preretinally. In a patient with an IOFB (a wire measuring 10.0 x 1.0 mm, at 20 mm from the anatomical axis, and 9-11.5 mm from the limbal plane) and local retinal detachment, there was a discrepance between the foreign body location indentified by radiography and that identified by CT with the use of the Komberg-Baltin prosthesis. Large differences in the distance between the IOFB and the limbal plane and between the IOFB and the anatomical axis (4 mm and 5 mm, respectively) were caused by the mobility of the foreign body located beneath the retina.
Conclusion: Localizing an IOFB using Komberg-Baltin prosthesis-assisted CT is advantageous to radiography due to an opportunity for accurate localization of a mobile IOFB with a patient in the position as similar as possible to his position during IOFB removal surgery (i.e., the supine position).
References
Mester V, Kuhn F. Intraocular foreign bodies. Ophthalmol Clin North Am. 2002 Jun;15(2):235-42. https://doi.org/10.1016/S0896-1549(02)00013-5
Mir TA, Canner JK, Zafar S, Srikumaran D, Friedman DS, Woreta FA. Characteristics of open globe injuries in the United States from 2006 to 2014. JAMA Ophthalmol. 2020;138(3):268-75. https://doi.org/10.1001/jamaophthalmol.2019.5823
Bourke L, Bourke E, Cullinane A, O'Connell E, Idrees Z. Clinical outcomes and epidemiology of intraocular foreign body injuries in Cork University Hospital, Ireland: an 11-year review. Ir J Med Sci. 2021 Aug;190(3):1225-30. PMID: 33230610. https://doi.org/10.1007/s11845-020-02443-9
Zhang Y, Zhang M, Jiang C, Qiu HY. Intraocular foreign bodies in china: clinical characteristics, prognostic factors, and visual outcomes in 1,421 eyes. Am J Ophthalmol. 2011 Jul;152(1):66-73.e1. https://doi.org/10.1016/j.ajo.2011.01.014
Vingopoulos F, Wang Y, Grob S, Li CYL, Eliott D, Kim LA, et al. Open Globe Injury with Intraocular Foreign Body. J Vitreoretin Dis. 2021 Jul 1;5(4):288-294. https://doi.org/10.1177/2474126420965033
Zhaboiedov GD, Kireiev VV. [Ophthalmology:Training]. Kyiv: Meditsina; 2012. Ukrainian.
Gor DM, Kirsch CF, Leen J, Turbin R, Von Hagen S. Radiologic Differentiation of Intraocular Glass: Evaluation of Imaging Techniques, Glass Types, Size, and Effect of Intraocular Hemorrhage. Am J Roentgenology. 2001 Nov;177(5):1199-203. https://doi.org/10.2214/ajr.177.5.1771199
Ulianova NA, Stasiuk IuV, Sidak-Petretska OS, Tychina NP. [Method of the x-ray localization of intraocular foreign bodies]. 116572, 2023.
Parke DW 3rd, Flynn HW Jr, Fisher YL. Management of intraocular foreign bodies: a clinical flight plan. Can J Ophthalmol. 2013 Feb;48(1):8-12. https://doi.org/10.1016/j.jcjo.2012.11.005
Jabłoński M, Winiarczyk M, Biela K, Bieliński P, Jasielska M, Batalia J, et al. Open Globe Injury (OGI) with a Presence of an Intraocular Foreign Body (IOFB)-Epidemiology, Management, and Risk Factors in Long Term Follow-Up. J Clin Med. 2022 Dec 26;12(1):190. https://doi.org/10.3390/jcm12010190
Jung HC, Lee SY, Yoon CK, Park UC, Heo JW, Lee EK. Intraocular Foreign Body: Diagnostic Protocols and Treatment Strategies in Ocular Trauma Patients. J Clin Med. 2021 Apr 25;10(9):1861. https://doi.org/10.3390/jcm10091861
Parke DW 3rd, Pathengay A, Flynn HW Jr, Albini T, Schwartz SG. Risk factors for endophthalmitis and retinal detachment with retained intraocular foreign bodies. J Ophthalmol. 2012;2012:758526. https://doi.org/10.1155/2012/758526
Downloads
Published
Issue
Section
License
Copyright (c) 2023 Ulianova N.A., Stasiuk, Iu.V., Sidak-Petretska O.S., Tychina N.P., Bondar N.I., Rodina Iu.M.

This work is licensed under a Creative Commons Attribution 4.0 International License.
This work is licensed under a Creative Commons Attribution 4.0 International (CC BY 4.0) that allows users to read, download, copy, distribute, print, search, or link to the full texts of the articles, or use them for any other lawful purpose, without asking prior permission from the publisher or the author as long as they cite the source.
COPYRIGHT NOTICE
Authors who publish in this journal agree to the following terms:
- Authors hold copyright immediately after publication of their works and retain publishing rights without any restrictions.
- The copyright commencement date complies the publication date of the issue, where the article is included in.
DEPOSIT POLICY
- Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) during the editorial process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
- Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the journal's published version of the work with an acknowledgement of its initial publication in this journal.
- Post-print (post-refereeing manuscript version) and publisher's PDF-version self-archiving is allowed.
- Archiving the pre-print (pre-refereeing manuscript version) not allowed.








